Article type: Report
20 September 2024
Volume 46 Issue 1
HISTORY
RECEIVED: 18 June 2024
REVISED: 30 July 2024
ACCEPTED: 4 August 2024
Article type: Report
20 September 2024
Volume 46 Issue 1
HISTORY
RECEIVED: 18 June 2024
REVISED: 30 July 2024
ACCEPTED: 4 August 2024
![]() Key elements to consider when choosing an assessment tool for understanding risk related to harmful sexual behaviours
Key elements to consider when choosing an assessment tool for understanding risk related to harmful sexual behaviours

Amanda J Paton1 MPsych(Applied), Deputy Director, Practice * 

Sian Burgess1 MPsych(Applied), Teaching Academic

Leah Bromfield1 PhD, Director
Affiliations
1 Australian Centre for Child Protection, University of South Australia, Adelaide, SA, Australia
Correspondence
*Mrs Amanda J Paton
Contributions
Amanda J Paton - Study conception and design, Acquisition of data, Analysis and interpretation of data, Drafting of manuscript, Critical revision
Sian Burgess - Analysis and interpretation of data, Critical revision
Leah Bromfield - Study conception and design
Amanda J Paton1 *
Sian Burgess1
Leah Bromfield1
Affiliations
1 Australian Centre for Child Protection, University of South Australia, Adelaide, SA, Australia
Correspondence
*Mrs Amanda J Paton
CITATION: Paton, A. J., Burgess, S., & Bromfield, L. (2024). Key elements to consider when choosing an assessment tool for understanding risk related to harmful sexual behaviours. Children Australia, 46(1), 3016. doi.org/10.61605/cha_3016
© 2024 Paton, A. J., Burgess, S., & Bromfield, L. This work is licensed under the terms of a Creative Commons Attribution 4.0 International Licence
Abstract
This paper takes a critical practice lens to examine the challenge of selecting a fit-for-purpose tool to assess children and young people who have displayed harmful sexual behaviours (HSB).
When assessing risk and complex behavioural or mental health concerns, we often turn to structured tools or protocols to guide and inform our thinking and decision making. The area of understanding risk in HSB is no different. However, practitioners and front-line workers often find themselves feeling ill prepared to make thorough assessments of wellbeing and risk of future harm related to a child or young person who has displayed HSB.
Blending practice-based wisdom and evidence-based literature, six key elements have been identified to help guide practitioners to select the right fit-for-purpose tool to support assessment of children and young people who have displayed HSB. These elements aim to provide guidance to practitioners to inform decision making about tool selection, ensuring that chosen tools are fit for purpose.
Keywords: assessing risk, child sexual abuse, harmful sexual behaviours, tools to assess risk of harm.
Background
Worldwide, children and young people’s harmful sexual behaviours (HSB) are a significant problem and, nationally, the high prevalence of HSB and sexual exploitation in institutional contexts has been highlighted as a growing concern (Bromfield et al., 2017; Gatwiri et al., 2020; National Society for the Prevention of Cruelty to Children, 2021; Royal Commission into Institutional Responses to Child Sexual Abuse, 2017). More recently, the Australian Child Maltreatment Study showed that this is not just an issue for institutional contexts, with approximately half of those individuals who reported experiencing child sexual abuse noting that the person responsible for the harm was another child or young person (Mathews et al., 2024).
In Australia, the National Office for Child Safety in consultation with the National Clinical Reference Group (NCRG), developed the following working definition of HSB (Attorney-General’s Department, 2023):
Harmful sexual behaviours are sexual behaviours displayed by children and young people that fall outside what may be considered developmentally expected or socially appropriate, may cause harm to themselves or others, and occur either face to face and/or via technology. When these behaviours involve others, they may include a lack of consent, reciprocity, and mutuality, and may involve the use of coercion, force, or misuse of power.
While the impacts of HSB may vary from child to child depending on their circumstances, life experiences and unique personal attributes, research suggests that some children and young people who have experienced sexual harm by another child or young person display many of the same trauma impacts as children sexually harmed by adults and are at risk of experiencing life-long impacts, including trauma (Shaw et al., 2000; O’Brien, 2010). Given this, it is common for there to be some form of assessment of future risk of HSB occurring (El-Murr, 2017). Generally, this assessment is to ascertain the level of concern, or not, those around the child or young person should have with regard to their behaviour, i.e., the likelihood of that behaviour occurring again (as often is the case in criminal justice settings) and the potential harm the child or young person may cause to other children in the future (as is often the case within clinical and out-of-home-care settings). For this assessment, we commonly turn to risk assessment tools and processes to guide decision making and understanding of likely risk.
Jensen et al. (2022) suggested that assessors need to understand a chosen tools’ psychometrics, strengths and limitations to ensure the most appropriate assessment tool is selected for the given setting and purpose and be mindful of the impact their assessment has on involved children and families. Risk assessment instruments need to be critically evaluated by practitioners using them and should, where possible, form part of broader comprehensive assessments, inclusive of developmental histories, contextual factors and the presence and influence of risk and protective factors in a child’s social and physical environment. The reliability and validity of tools and processes is important to the selection process; however, it is also important for tools and processes to be used within their designed purpose and validated scope (Gotch & Hanson, 2016).
Assessing risk in children and young people demands a high degree of responsibility because outcomes have profound impacts, such as informing placement decisions, level of supervision/restriction imposed and selection of appropriate treatments (Allardyce & Yates, 2018; Prentky & Righthand, 2003). Acknowledging that the choice of a particular tool over another is influenced by various factors, including practitioners needing to adhere to organisational policies and requirements of pre-selected tools, it is important to understand the relevance of individual risk and protective factors, the significance of the unique context of behaviours and the validity and limitations of assessment tools.
Considering the significant impact of these assessments, how can practitioners select the right tool for the right purpose, context and for the individual characteristics of the individual child or young person? We used an evidence-informed practice approach to answer this question and develop a set of key elements to guide practitioners’ use of tools and processes when assessing risk for children and young people who have displayed HSB.
Blending practice-based expertise with evidence-based literature
Drawing on the evidence-based literature from a scoping review by G. Horch, S. Cox, A. Paton, J. Krakouer and L. Bromfield (unpubl. data), articles and risk tools were identified, summarised and discussed in a series of five workshops led by one of the co-authors, lasting in duration from 45 to 150 mins, and including three to five practice experts (some co-authors from the present article). Members included in the practice-based expert group were psychologists and clinical psychologists with: extensive expertise (5–20 years’ experience) in the assessment and treatment of children, young people and adults impacted by sexual violence, including child sexual abuse and children and young people who had displayed HSB; experience in both the clinical therapeutic and forensic contexts; responsibility for the clinical supervision and governance of teams of therapeutic practitioners; extensive experience developing and managing service responses including the selection, purchase and administration of a range of psychometric assessment tools, including those commonly used to assess and understand HSB; and experience in the training of practitioners to use such tools and undertake thorough assessments.
All the practice experts who contributed their expertise to these discussions were members of the Australian Centre for Child Protection (ACCP) at the University of South Australia. A participatory action research-style approach was applied to the development of this practice tool to ensure practice knowledge was considered alongside available literature. Given the practice-based approach, no formal ethics approvals were required and all practice experts contributed as part of their role within the ACCP.
During these workshops, key elements or criteria emerged that each member considered when reviewing tools to decide their suitability. Specifically, members were interested in information regarding the purpose of the tool or process, the evidence base for their use, if they included dynamic and protective factors, inclusion of technology-assisted HSB considerations, the use of language, theoretical underpinning, use of risk categorisations, considerations about the heterogeneity of HSB populations, cultural safety and considerations about user requirements and costs of its use. These elements were subsequently refined and consolidated alongside the literature on assessing risk in children and young people who have displayed HSB by a second co-author (and member of the expert group). Draft key elements were tested further with members of the expert practice group and refinements made accordingly. The elements were then tested against a series of tools highlighted in the scoping review for practical utility and refinements were made again to the final six key elements.
Selecting the right assessment tool
Six key elements should be considered individually and in combination with one another to select the correct tool when assessing children and young people who have displayed HSB (see Figure 1). Whilst a thorough and holistic clinical assessment is essential, inclusion of findings from robust assessment tools can help practitioners make decisions, plan for future therapeutic interventions and guide understanding of risk and how to enhance safety if these are selected and used correctly.
Figure 1. How to select the right tool to assess risk for children and young people who have displayed harmful sexual behaviour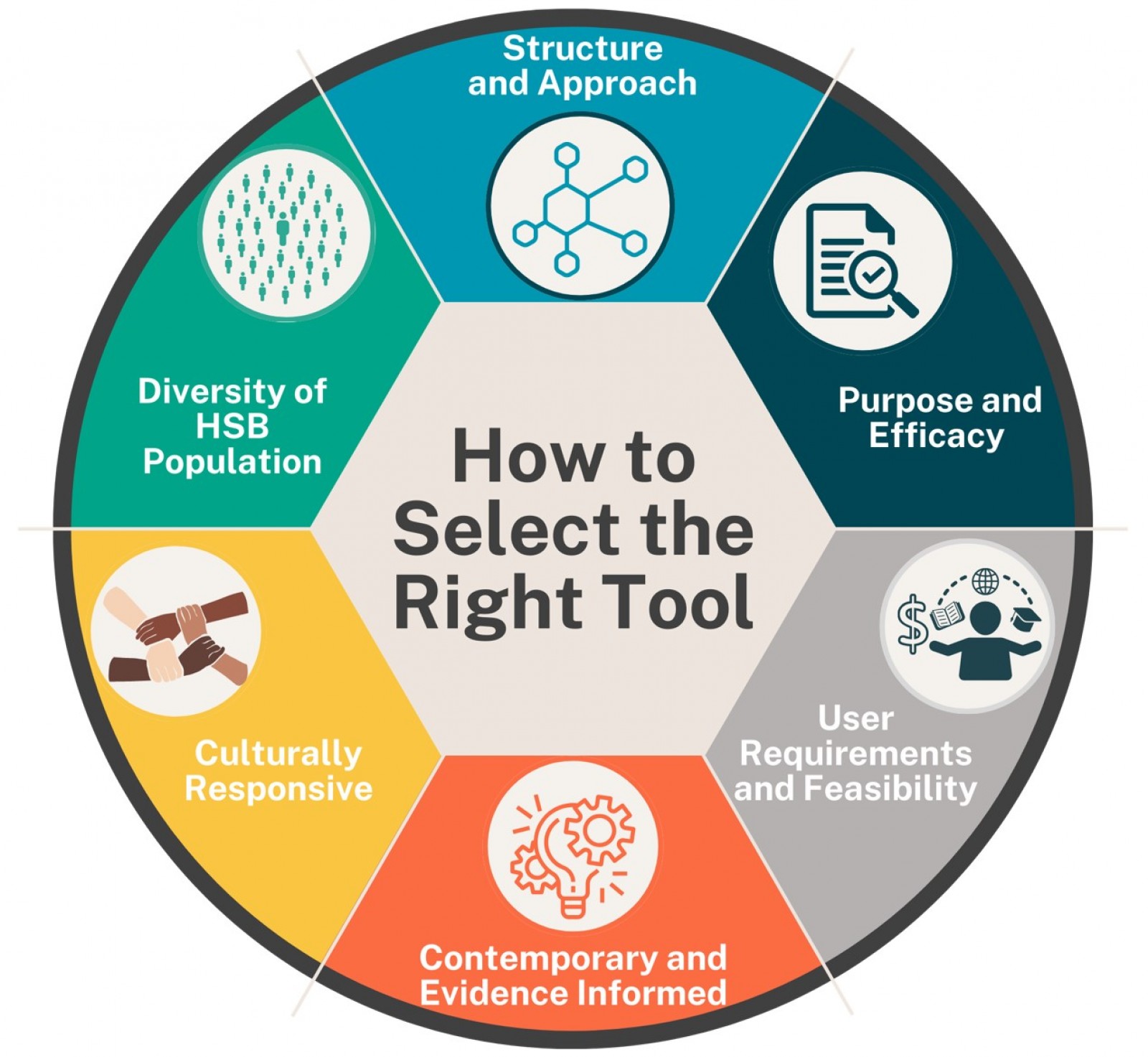
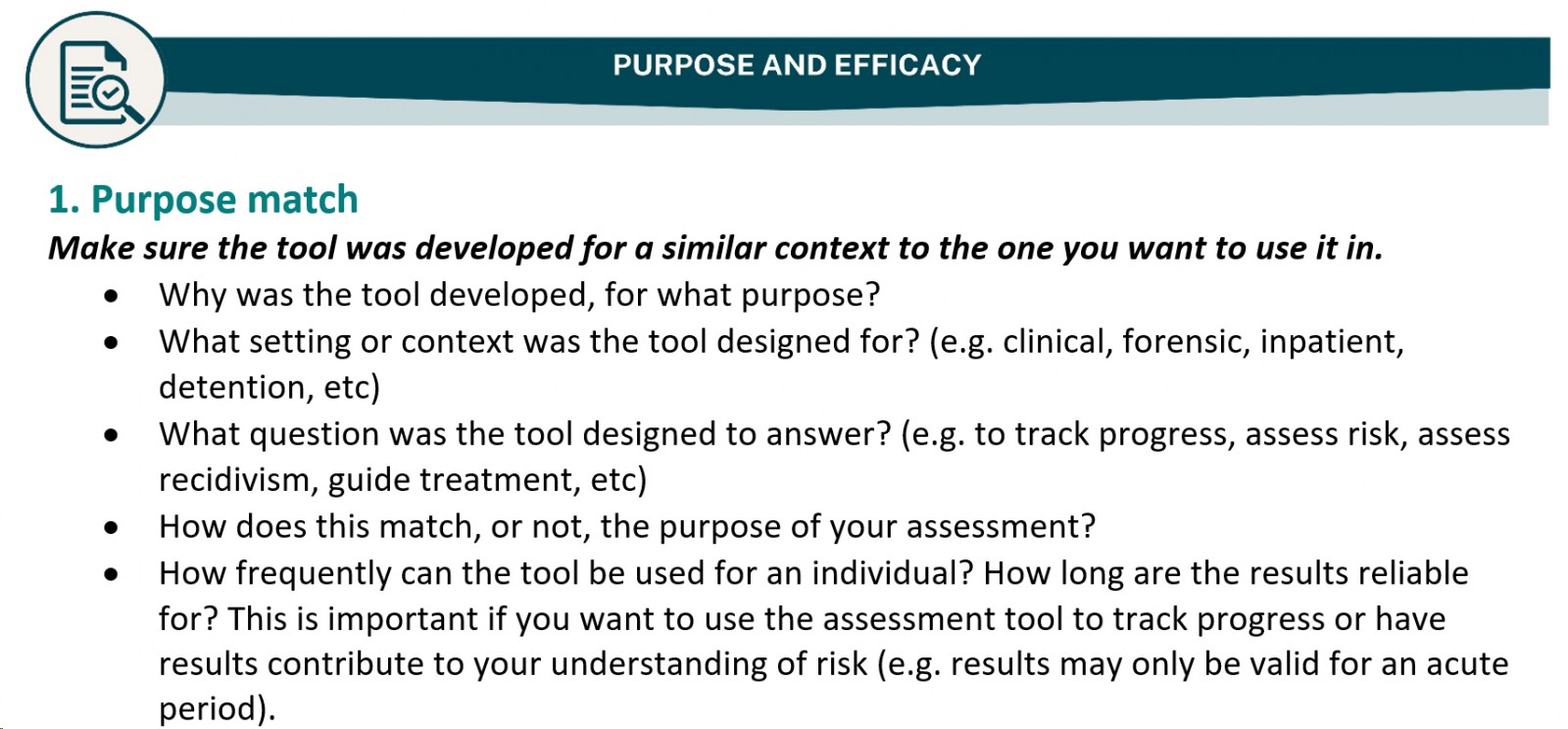
1. Purpose and efficacy
Purpose of the assessment tool
It is crucial for anyone who uses risk assessment tools to be clear on the purpose of the assessment and how this aligns (or not) with the designed purpose of any proposed tool. It is important to keep in mind that forensic settings are distinctly different from clinical or child protection settings, and each setting requires different skill sets in practitioners and different tools that are matched to the purpose of the setting. For example, a forensic assessment may be more concerned with recidivism, whereas a clinical setting may be more interested in treatment needs and outcomes as treatment progresses. The choice of tool should therefore depend on the setting and the purpose of the risk assessment (Gotch & Hanson, 2016).
Within forensic settings, where sexual recidivism is important, the accuracy of predictions amongst tools is critical; unfortunately, there is significant variability in the validity of tools for specific context, target age and adjudication status (Jung & Thomas, 2022; Miccio-Fonseca, 2023). Within child protection and clinical contexts, the assessment needs may extend further than assessing sexual recidivism risk and may include the need to identify treatment targets and monitor intervention progress. For these circumstances, measuring dynamic risk and protective factors is more important than static risk factors (Kang et al., 2019; Worling, 2020).
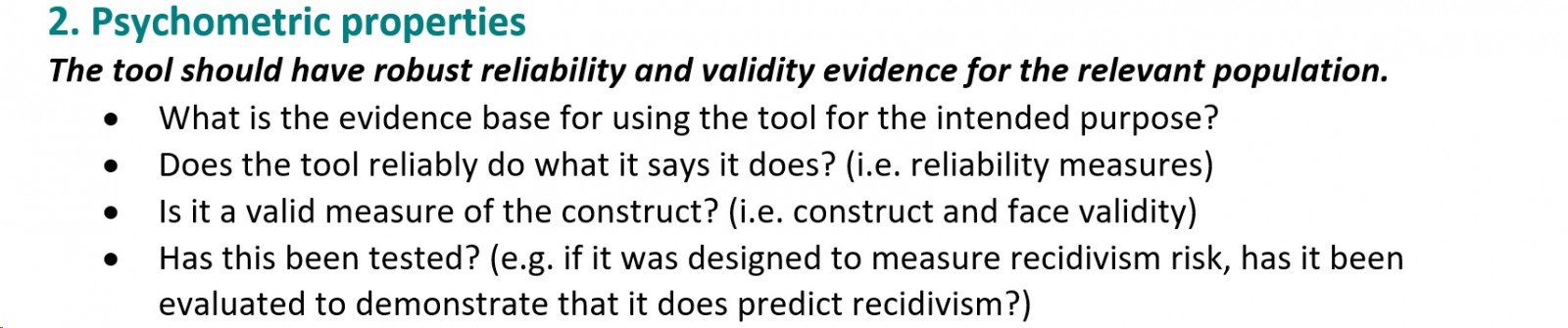
Psychometric properties
Fernandez and Delfabbro (2020) suggested that the quality of any assessment tool is determined by its reliability and validity, i.e. how consistent is it in measuring items, does it measure what it is supposed to measure and how well does it measure what it is supposed to measure. Most tools have information available on a range of reliability and validity measures; the most common measure of reliability is Cronbach’s alpha, which measures how consistently a measure will give the same result (Tavakol & Dennick, 2011). Generally, a higher alpha coefficient is good (e.g. above 0.70) and tools with an alpha below this should be used with caution. However, some tools may have good overall alpha values (e.g. above 0.70) but several individual scales may have poor alpha values (e.g. below 0.50). Tools with limited items or those that have used a small sample size to set a baseline may also have a lower-than-expected alpha (Taber, 2017). Interpretation of alphas and other measures can be complex and, therefore, care should be taken when reviewing tools. We suggest reviewing multiple reference points for reliability and validity.
In addition to measures of reliability and validity, standardised tests or tools should have clearly defined norms that reflect the target group for which the test/tool was designed. This should be set on the basis of a large representative sample of the population and clearly noted in the tools’ user manuals or guidelines (American Psychological Association (APA), 2023).
Even if risk assessment tools are robust and independently validated, professionals frequently fail to consider the context of research findings, limitations and disagreement between studies when selecting and using risk assessment tools (Allardyce & Yates, 2018; Miccio-Fonseca, 2023; Myers, 2007). A practitioner’s critical review of a tool needs to extend past face validity and reliability measures and consider the more detailed metrics and construction of the tool, including scores and weightings. For example, very few tools have baseline data on the prevalence of specific items for specific populations, so the reduced value of measuring items without having baseline data with which to compare needs to be considered.
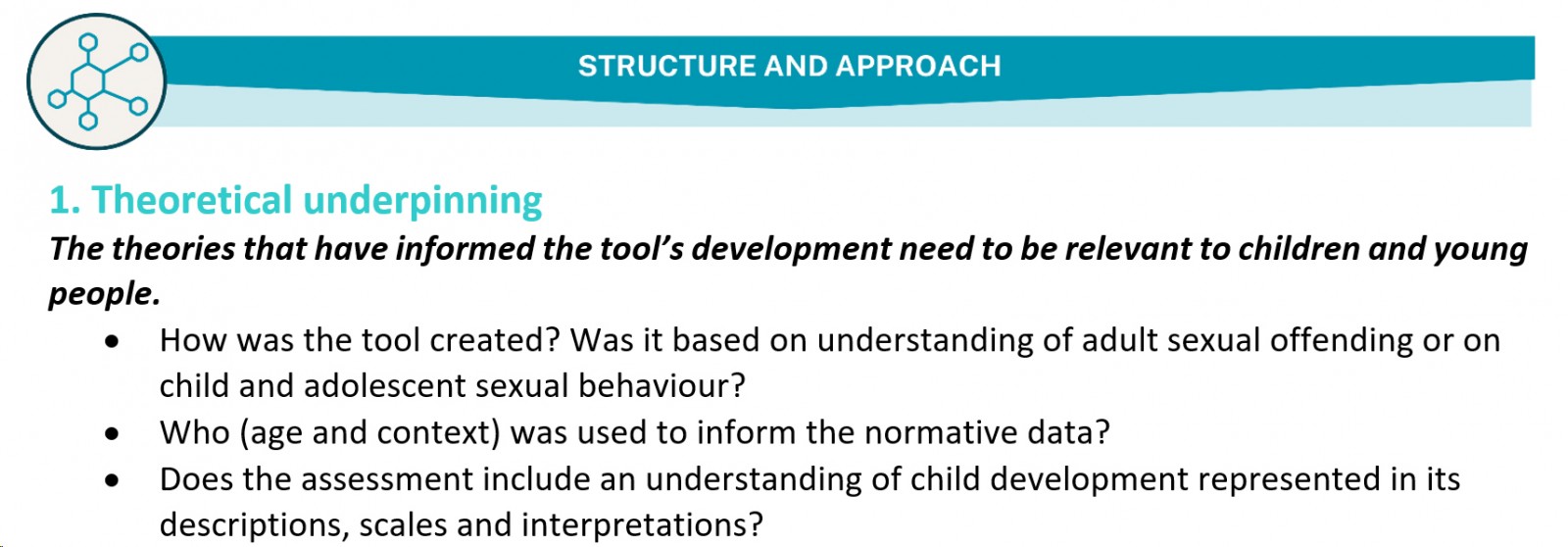
2. Structure and approach
Theoretical underpinning – adult versus child paradigm
When assessing risk for children and young people who have displayed HSB, it is important to consider the developmental divide between childhood and adulthood and the distinct aetiologies of HSB relative to adult sexual offending. HSB risk assessment tools based on adult-centred risk prediction fail to acknowledge significant biological, neurological, psychological and social changes throughout childhood and adolescence. Historically, the development of risk assessment tools for sexualised behaviour has been focused on adult male forensic populations and tools for assessing risk in adolescent populations were initially based on, or adapted from, these adult risk assessment tools. Many HSB risk assessment measures have been downward extensions of adult counterparts and subsequent youth-related versions have often been enmeshed with empirical literature based on male adult convicted sex offenders without questioning their validity for children or young people (Miccio-Fonseca, 2023; Vitacco et al., 2009). The widely used ERASOR 2.0, for example, has been withdrawn by its developer because its development was based on adult risk assessment tools and some risk factors were not deemed appropriate for predicting sexual recidivism of adolescents (Miccio-Fonseca & Rasmussen, 2018; Worling, 2017).
The application of adult findings to children and young people is concerning, with adult risk factors often being unrelated to juvenile sexual recidivism (Powers-Sawyer & Miner, 2009). Further, known risk or protective factors for one age group may not accurately assess risk in another age group, so an understanding of how these differ across age groups and fluctuate depending on current functioning is essential (Awrey, 2021; Miccio-Fonseca & Rasmussen, 2018; Van Der Put et al., 2011). The Association for the Treatment and Prevention of Sexual Abuse (ATSA) continues to highlight the fundamental difference between children, adolescents and adults who engage in HSB and continues to demand the use of developmentally appropriate assessment and intervention approaches relevant to the purpose of the evaluation and specifically tailored for the individual who is being assessed (Association for the Treatment of Sexual Abusers (ATSA), 2023; Gotch & Hanson, 2016).
Given this, tools designed and validated for adult perpetrators of child sexual abuse, or those that heavily draw on adult tools, should not be used with children and young people who have displayed HSB. Even those who have been adjudicated for sexual offences require tools designed and validated for use with children and young people.
Inclusion of dynamic, protective, and contextual factors
Aligned with elements noted in the Association for the Treatment & Prevention of Sexual Abuse (ATSA) report (2023), it is preferable that tools including consideration of broader contextual factors, and a child or young person’s strengths and protective factors, be chosen for use with children and young people who have displayed HSB. Evidence suggests the inclusion of strengths and protective factors in comprehensive risk assessments adds value to recidivism predictions, intervention planning and risk management (Allardyce & Yates, 2018; Langton et al., 2023). Assessments of risk should consider predisposing and protective factors across all aspects of the child’s life to accurately determine treatment targets and mitigate the effect of risk.
Historic and static factors that have contributed to the development of HSB cannot be altered by interventions and fail to account for rapid changes in developing children and young people, which are better accounted for by dynamic factors. Therefore, risk assessment tools for children and young people must include both static and dynamic risk factors. Measures that can assess change and include dynamic variables move beyond mere predictions of recidivism and by combining risk and protective factors, the predictive validity of assessment tools can be improved (de Vries Robbe, 2014; Rojas, 2013). Risk assessment instruments that include dynamic risk factors can also provide valuable information for treatment targets.
Key considerations when assessing HSB are the physical (face-to-face) and virtual (digital) context of the behaviour, relationships between settings and developmental factors of the child, to understand how environmental context can trigger behaviours and what changes may be necessary within the environment to prevent HSB (ATSA, 2023; Navarro & Tudge, 2022). Understanding how risk-related items are relevant to the specific contextual and individual factors is crucial. Although many factors are associated with risk, the reason why an individual persists with a behaviour may be very different from the reasons relating to the emergence of the behaviour (Allardyce & Yates, 2018).
Use of levels of concern
The level of risk varies considerably between children with HSB, and risk categorisations are widely used; however, several concerns have been raised in the literature and by practitioners about categorising children into low, medium or high risk. The concerns are twofold: one is about how the risk categories of some tools have been established and what they communicate and the second is whether there should be categories at all (Allardyce & Yates, 2018; Davies et al., 2022; Miccio-Fonseca & Rasmussen, 2015). Risk categories often lack statistical basis and normative data, bringing uncertainty to the meaning that ‘high risk’ or ‘significant concern’ conveys: it is important to consider whether there is an evidence base to support adding up scores at equal weights and determining risk categories without statistically derived cut-off scores.
Considering that a cut-off score determines an arbitrary risk category that often determines a system response, assessors need to question the actual difference in risk between a young person being classified as ‘moderate risk’ or ‘high risk’, for example. Rather, understanding the presence of specific risk factors and their relevance to risk for sexual violence may provide better guidance than a risk score (Hart & Boer, 2021). Risk assessment tools that categorise children into low, medium or high risk can result in arbitrary administrative decisions with little guidance for risk management and placement decisions and little consideration of risks to specific children or young people in particular settings (Allardyce & Yates, 2018; Kang et al., 2019). Despite training requirements for the use of some risk assessment tools, there are vast differences with how individual assessors interpret arbitrary risk categories and assign children to a category.
3. Diversity of HSB population
It is important to understand that children who have displayed HSB are not a homogeneous group. They are a diverse and complex population that are often not adequately represented/considered in the creation of assessment tools. Risk assessment research has primarily focused on adjudicated male adolescents of mainstream intellectual ability (Miccio-Fonseca & Rasmussen, 2020; Worling & Langton, 2012). Variances in gender, developmental stages, intellectual functioning and age need to be considered when evaluating risk and protective factors over time, so risk assessment tools need to be tailored to the population assessed and psychometric measures need to be aligned to the culture, language and context in which they are used (Miccio-Fonseca & Rasmussen, 2018). It may not be feasible to develop and validate assessment tools for each potential subgroup; however, risk assessments are susceptible to bias based on diversity, including age, gender, ethnicity and abilities, so assessors need to be able to identify and appropriately consider diversity in risk assessments.
Age considerations
Risk assessments are potentially susceptible to bias based on age, encompassing factors such as development or maturity (Hart & Boer, 2021). It is concerning that risk assessment tools developed for adults are used to evaluate adolescents and tools developed for adolescents are used to evaluate children. Applying knowledge of adolescent HSB risk factors to children could be detrimental to identification and treatment efforts, so adolescent risk assessment protocols and variables should not be used to assess risk of children who have displayed HSB. Miccio-Fonseca (2018) identified age differences in risk and protective factors for children with HSB. Further, there is evidence that the predictive validity of individual risk factors changes, and the effects of protective factors vary, as children grow older, which underscores the need for researching developmentally specific risk and protective factors (Van Der Put et al., 2011; Worling & Langton, 2012).
Gender and sexuality considerations
Risk assessment tools are also susceptible to bias based on gender, encompassing factors such as biological sex, gender identity, gender role, gender expression and sexual interest. It is concerning that risk assessment tools developed for male adolescents are assumed to be applicable and used with children and young people with diverse genders and developing sexual interests.
The research into transgender young people and HSB is extremely limited, although reported rates appear extremely low. There are some clear gender differences in risk and protective factors in children and young people who have displayed HSB, so risk assessment tools need to be gender-sensitive to prevent inappropriate conclusions being drawn regarding risk, intervention targets or placement decisions; in the absence of this, assessors must apply caution when interpreting results of some tools.
Ability considerations
Risk assessments are also potentially susceptible to bias based on physical, cognitive or mental ability differences. Children and young people with low intellectual functioning are consistently over-represented in cohorts of children who have displayed HSB and score significantly higher on risk-scale scores (Allardyce & Yates, 2018; Hackett et al., 2013; Miccio-Fonseca & Rasmussen, 2020; Seto & Lalumiere, 2010). It is concerning that risk assessment tools developed for adolescents with mainstream abilities are used with children and young people with diverse abilities and should be avoided, or at least interpreted with caution, by assessors.
Miccio-Fonseca and Rasmussen (2020) highlighted that young people with intellectual challenges who have displayed HSB differ in several ways from young people with mainstream abilities. This population may not understand the harmful nature of their behaviours; they are more likely to harm opportunistically and impulsively; they are less likely to use grooming techniques; and lower scores on their protective scales suggest higher rates of social isolation and the need for interventions to improve their resources (Hackett, 2014; Miccio-Fonseca & Rasmussen, 2018). Assessments of this population should therefore be sensitive to the psychosocial environment of a child or young person, as well as their intellectual and psychological functioning. Assessors need to be aware of variations in socio-emotional, physical and cognitive development between children of the same biological age and risk assessment tools need to be developmentally sensitive and applicable to young people with diverse abilities.
4. Culturally responsive
In addition to gender and age, risk assessments are also potentially susceptible to bias based on ethnicity, encompassing factors such as race, culture, nationality, language, religion or other aspects of heritage (Hart & Boer, 2021). Historically, risk assessment tools were developed based on paradigms associated with adjudicated male adolescents or adults from western cultures, predominantly the United States of America, Canada or the United Kingdom. Although some risk assessment tools have ethnically diverse validation samples and demonstrate reasonable results for predictive validity (Barroso et al., 2019; Rojas & Olver, 2020), these tools do not always address considerations for cultural safety and potential racial biases (Fix et al., 2017; Childs et al., 2022; Molnar et al., 2022). For example, Molnar et al., (2022) noted that the Juvenile Sex Offender Management Protocol-II (J-SOAP-II) had poor predictive value for sexual recidivism for both Indigenous and non-Indigenous young people in an Australian sample, despite having included cultural variability within the tool’s normative data during development. Jung and Thomas (2022) highlighted the lack of empirical data for HSB risk assessment tools for First Nations children and young people and the risk of bias and unfairness when assessing risk of First Nations populations with tools that have not been developed by, or co-designed with, First Nations populations.
Aboriginal and Torres Strait Islander children and young people
Aboriginal and Torres Strait Islander children and young people continue to be overrepresented in the Australian out-of-home care (OOHC) context; the latest data released by the Productivity Commission (2023) showed that 43.7% of children in OOHC are Aboriginal and Torres Strait Islander children.
Considering that higher proportions of Aboriginal and Torres Strait Islander children continue to enter OOHC than non-Aboriginal children, and they remain in OOHC for longer periods, they are more likely to be in an institutional environment that puts them at risk of institutional child sexual abuse, including HSB (Anderson et al., 2017; Liddle et al., 2022). Potential cultural bias, transgenerational impacts of colonisation upon Aboriginal children and a lack of understanding of Aboriginal culture need to be addressed as part of decolonising practice when striving towards culturally competent assessments (Adams et al., 2014; Black et al., 2018). This raises the concern of the impact of using tools designed for non-indigenous forensic populations with First Nations children and young people.
The Principles of Practice in Mental Health Assessment with Aboriginal Australians (Adams et al., 2014) and work by the Centre of Best Practice in Aboriginal and Torres Strait Islander Suicide Prevention (CBPATSISP) provide some key considerations for selecting and using culturally appropriate assessment tools. The CBPATSISP Clearing House shares promising and best practice resources, guidelines, research, programs and services for use with Aboriginal and Torres Strait Islander people and provides examples of culturally safe assessment tools approved by the CBPATSISP that may be relevant for practitioners to consider.
Although practitioners are encouraged to seek additional cultural advice and support from relevant Aboriginal cultural advisors and/or Aboriginal Community Controlled Organisations to support their practice and decision making when working with Aboriginal children and young people, the materials highlighted by CBPATSISP suggest key questions an assessor should consider, including: What is the purpose of using the tool? Is the tool culturally appropriate? Has the tool been validated for use with Aboriginal and Torres Strait Islander people? What is a culturally safe assessment process and is the tool being used in a culturally safe environment? Is the person who uses and interprets the results culturally competent and culturally sensitive? Is it appropriate for the person who uses the tool to be of a different gender than the Aboriginal child who is being assessed? (Westerman, 2010).
5. Contemporary and evidence informed
Understanding of HSB displayed by children and young people is a continually evolving field of research and practice. Terms such as ‘juvenile sex offender’ were once readily used and those children and young people who displayed HSB towards other children were considered similar to adult child sexual offenders, requiring the same punishments, responses and management to ensure community safety. We now approach and understand the aetiology of these behaviours differently and subsequently apply a more measured and matched response to the level of behaviour, concern and harm. Similarly, issues including exposure to pornography and the use of technology to facilitate HSB were not factors readily considered 10 years ago. Today, however, pornography and technology feature heavily in our contemporary understanding of HSBs. It is therefore crucial to review the contemporary evidence used to inform a tool’s development when considering its use, and to ensure these newer elements are considered.
Inclusion of technology-assisted (TA) HSB
The term technology-assisted harmful sexual behaviour (TA-HSB) refers to online and offline aspects of HSB that use the internet and/or any image-creating/sharing or communication device. Behaviour may include one or more children engaging in sexual discussions or acts that are considered inappropriate and/or harmful given their age or stage of development (Allotey & Swann, 2019; Hackett et al., 2019).
In Australia, referral data for an HSB treatment program indicated 65% of male referrals and 80% of female referrals involved TA-HSB (McKillop, 2018). Despite the prevalence of TA-HSB, most existing assessment tools and processes fail to include relevant considerations. Because of the lack of TA-HSB considerations in most existing tools and processes, and the likely prevalence of TA-HSB in many clinical samples, it is imperative to explore TA-HSB aspects together with offline HSB as part of comprehensive risk assessments.
Considering use and exposure to pornography
Developmentally inappropriate use of pornography has been identified as a potential trigger for development of HSB and can impede a young person’s ability to build healthy relationships (Belton & Hollis, 2016; Greater Manchester Safeguarding, 2022). In line with previous research, the use of pornography was found to cluster with other risk factors and accelerated the onset of HSB; however, contrary to previous research, even in the absence of other risk factors, the use of pornography was found to be related to HSB development (ATSA, 2020; McKibbin et al., 2022). Children who disclosed exposure to pornography were significantly more likely to disclose engaging in HSB and children exposed to pornography at a younger age were more likely to reach the threshold of clinically significant trauma (Dillard et al., 2019).
Including the use of assessment tools that have items related to pornography use is therefore critical considering the prevalence of pre-adolescent and adolescent exposure to pornography and associated risks for developing HSB.
Use of language
In the past, responses to children who have displayed HSB have been shaped by responses to adult sex offenders and children were inappropriately labelled on the basis of their behaviours (Paton et al., 2022). The use of criminalising terminology for children who have displayed HSB unnecessarily mislabels and stigmatises often deeply troubled children (Nolan, 2017). Although empirical and grey literature continue to use stigmatising language at times, there has been a noticeable shift in language used within HSB-related risk assessment tools. For example, from the Juvenile Sex Offender Management Protocol-II (J-SOAP-II), created in 2003 to the less labelling language of the 'Youth Needs and Progress Scale' (YNPS) in 2020 which was created by the same authors (Prentky & Righthand, 2003; Righthand et al., 2020). The name of assessment tools, and the language used for assessment items within the tools, is based on the cultural context and contemporary knowledge accessed at the time of its development and can provide an indication of any recognition of children’s psychosocial immaturity, developmental variability and susceptibility to exploitation that was considered. The language of risk assessment tools for children and young people and the language used during risk assessments should acknowledge that children and young people are still developing their sense of identity and that their cognitive capacity and emotional maturity is distinctly different from adults (Paton et al., 2022).
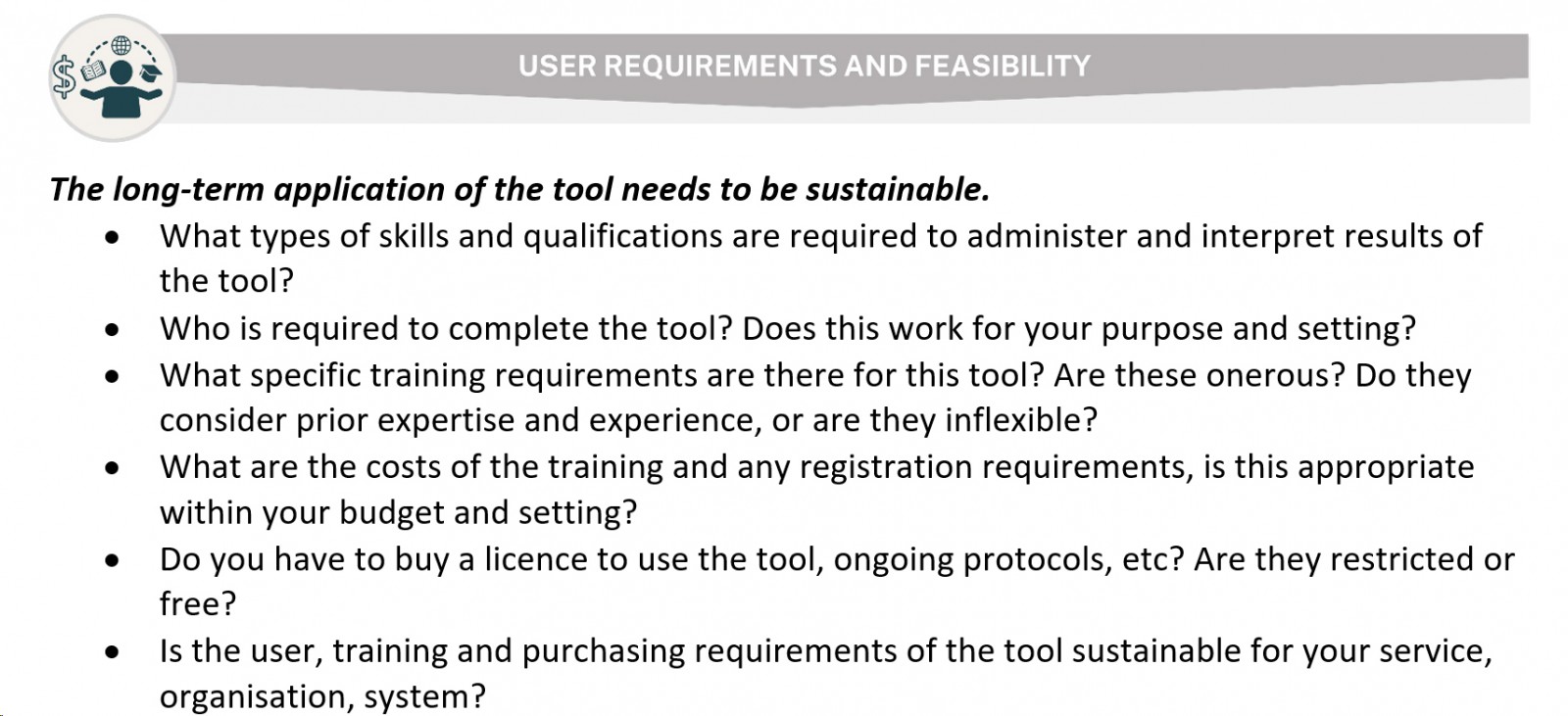
6. User requirements and feasibility
Undertaking risk assessments of children and young people who have displayed HSB requires special skills, knowledge and training. ATSA (2023) noted that complex assessments of children and young people who have displayed HSB should be conducted by qualified mental health professionals who are licensed in accordance with local laws and specific to their discipline with solid understanding of assessment and treatment of children with HSB. For many tools, there are user requirements to purchase the tool, and to administer and interpret the results, so it is important that professionals only use tools for which they are qualified and trained, including a thorough understanding of the instrument’s manual and adherence to appropriate application and interpretation of the tool. Even if a valid risk assessment tool has been appropriately selected for its context, the tool needs to be used by skilled, well trained, motivated and supported evaluators who have access to peer review processes, clinical supervision and administrative support for accurate and timely assessments (Gotch & Hanson, 2016). Some tools and processes are freely available online with no associated cost, some are freely available and have an associated training cost and others are restricted with licenses, subscriptions, required purchase of resources and mandatory training. Organisations need to consider the feasibility of required training, qualifications, the cost for accessing and implementing the tools and processes when making selections.
Summary
The emergence of HSB among children and young people represents a pressing concern, often indicative of significant adversity and complex needs. The enduring and widespread impacts of HSB underscore the necessity for accurate assessment to identify elements of risk associated with the behaviour and enhance mechanisms of safety. However, many existing measures of risk have not been adequately developed or evaluated for children and young people, leading to challenges in assessment accuracy. Additionally, practitioners may misuse tools beyond their intended scope or expertise. This article addresses these challenges by defining six key elements for selecting appropriate risk assessment measures. Drawing from both evidence-based literature and practical expertise, these elements offer a semi structured framework for critically evaluating HSB risk assessment tools tailored to individual needs. Such guidance serves experienced and new practitioners alike, facilitating the nuanced selection of assessment tools amidst the multifaceted nature of HSB while leveraging practitioner expertise for informed decision making.
Acknowledgements
We thank Dr Nada Ibrahim and Gina Horch for their contributions during early phases of the scoping review. Special thanks go to the following Practice Team and Research Team members for their invaluable contributions during workshops and iterative processes in the analysis phase of associated publications: Jacqueline Le Mesurier, Dr Sarah Shihata and Dr Eden Thain.
Funding statement
The researchers acknowledge the Western Australian Department of Communities who provided funding for this project under the Harmful Sexual Behaviours Solutions Project.
References
Adams, Y., Drew, N., & Walker, R. (2014). Principles of practice in mental health assessment with Aboriginal Australians. In P. Dudgeon, H. Milroy & R. Walker (Eds). Working together: Aboriginal and Torres Strait Islander mental health and wellbeing principles and practice. (pp. 271–288). Canberra: Commonwealth of Australia. thekids.org.au https://www.thekids.org.au/globalassets/media/documents/aboriginal-health/working-together-second-edition/wt-part-4-chapt-16-final.pdf
Allardyce, S., & Yates, P. (2018). Working with children and young people who have displayed harmful sexual behaviour. Edinburgh, Scotland: Dunedin Academic Press. DOI https://doi.org/10.2307/jj.12639024
Allotey, J., & Swann, R. (2019). Technology-assisted harmful sexual behaviour: Practice guidance. 2nd edn. London, UK: The AIM Project & NSPCC.
American Psychological Association (APA). (2023). Standardized test. In APA Dictionary of psychology. Washington, DC, USA: American Psychological Association. dictionary.apa.org https://dictionary.apa.org/standardized-test
Anderson, P., Bamblett, M., Bessarab, D., Bromfield, L., Chan, S., Maddock, G., Menzies, K., O’Connell, M., Pearson, G., Walker, R., & Wright, M. (2017). Aboriginal and Torres Strait Islander children and child sexual abuse in institutional contexts. Report for the Royal Commission into Institutional Responses to Child Sexual Abuse. Sydney: Commonwealth of Australia. apo.org.au https://apo.org.au/node/98086
Association for the Treatment and Prevention of Sexual Abusers (ATSA) Task Force on Children with Sexual Behavior Problems. (2023). Children with sexual behavior problems. 2nd edn. Beaverton, OR, USA: Association for the Treatment & Prevention of Sexual Abuse. members.atsa.com https://members.atsa.com/ap/CloudFile/Download/pgGxjO4p\
Association for the Treatment & Prevention of Sexual Abuse (ATSA). (2020). Understanding and responding to pornography use among adolescents who have engaged in sexually abusive behavior: Facts and considerations for practice. Beaverton, OR, USA: Association for the Treatment & Prevention of Sexual Abuse. members.atsa.com https://members.atsa.com/ap/CloudFile/Download/P2D02Yqr#:~:text=•%20Responses%20to%20pornography%20use%20must%20be%20realistic.&text=Therapeutic%20responses%20to%20pornography%20use,build%20healthy%20sexual%20self-regulation\
Attorney-General’s Department. (2023). National Strategy to Prevent and Respond to Child Sexual Abuse (2021–2030): First Annual Report 2023. Canberra: Australian Government. childsafety.gov.au https://www.childsafety.gov.au/system/files/2023-12/first-annual-report-national-strategy-2023.PDF
Awrey, M. (2021). Predicting recidivism versus desistance in adolescents with sexual offenses using tools developed for adults: The Static-99 and SAPROF. MA Thesis. Windsor, ON, Canada: University of Windsor. proquest.com https://www.proquest.com/openview/0b6a4fd085182ca579079755214b7dd9/1?pq-origsite=gscholar&cbl=18750&diss=y
Barroso, R., Pechorro, P., Ramiao, E., Figueiredo, P., Manita, C., Goncalves, R. A., & Nobre, P. (2019). Are juveniles who have committed sexual offenses the same everywhere? Psychometric properties of the Juvenile Sex Offender Assessment Protocol-II in a Portuguese youth sample. Sexual Abuse, 32(7), 806–825. DOI https://doi.org/10.1177/1079063219858070 PMid:31221049
Belton, E., & Hollis, V. (2016). A review of the research on children and young people who display harmful sexual behaviour online. NSPCC Impact and Evidence series. London, UK: NSPCC. learning.nspcc.org.uk https://learning.nspcc.org.uk/media/1198/review-children-young-people-harmful-sexual-behaviour-online.pdf
Black, E. B., Toombs, M. R., & Kisely, S. (2018). The cultural validity of diagnostic psychiatric measures for Indigenous Australians. Australian Psychologist, 53(5), 383–393. DOI https://doi.org/10.1111/ap.12335
Bromfield, L., Hirte, C., Octoman, O., & Katz, I. (2017). Child sexual abuse in Australian institutional contexts 2008–13: Findings from administrative data. Australian Centre for Child Protection. Sydney: Royal Commission into Institutional Responses to Child Sexual Abuse. childabuseroyalcommission.gov.au https://www.childabuseroyalcommission.gov.au/sites/default/files/file-list/research_report_-_child_sexual_abuse_in_australian_institutional_contexts_2008-13_findings_from_administrative_data_-_causes.pdf
Childs, K. K., Peck, J. H., & Brady, C. M. (2022). Predictive bias in juvenile risk assessment: Considering race/ethnicity and sex. Crime & Delinquency, 70(3), 1034–1059. DOI https://doi.org/10.1177/00111287221143936
Davies, S. T., Helmus, L. M., & Quinsey, V. L. (2022). Improving risk communication: Developing risk ratios for the VRAG-R. Journal of Interpersonal Violence, 37(1–2), 835–862. DOI https://doi.org/10.1177/0886260520914555 https://pubmed.ncbi.nlm.nih.gov/32316828.
de Vries Robbé, M. (2014). Protective factors: Validation of the structured assessment of protective factors for violence risk in forensic psychiatry. PhD Thesis. Nijmegen, Netherlands: Radboud University. irp-cdn.multiscreensite.com https://irp-cdn.multiscreensite.com/f430bf1b/DESKTOP/pdf/phd+thesis+protective+factors.+michiel+de+vries+robbe.pdf
Dillard, R., Maguire-Jack, K., Showalter, K., Wolf, K. G., & Letson, M. M. (2019). Abuse disclosures of youth with problem sexualized behaviors and trauma symptomology. Child Abuse & Neglect, 88, 201–211. DOI https://doi.org/10.1016/j.chiabu.2018.11.019 PMid:30537621
El-Murr, A. (2017). Problem sexual behaviours and sexually abusive behaviours in Australian children and young people: A review of available literature. Child Family Community Australia Paper No. 46. Melbourne: Australian Institute of Family Studies. aifs.gov.au https://aifs.gov.au/sites/default/files/publication-documents/46_problem_sexual_behaviours_0.pdf
Fernandez, E., & Delfabbro, P. (2020). Child protection and the care continuum: Theoretical, empirical and practice insights. London, UK: Routledge. DOI https://doi.org/10.4324/9781003121305
Fix, R. L., Cyperski, M. A., & Burkhart, B. R. (2017). Disproportionate minority contact: Comparisons across juveniles adjudicated for sexual and non-sexual offenses. Sexual Abuse, 29(3), 291–308. DOI https://doi.org/10.1177/1079063215601436 PMid:26297505
Gatwiri, K., Cameron, N., McPherson, L., & Parmenter, N. (2020). What is known about child sexual exploitation in residential care in Australia? A systematic scoping review. Children and Youth Services Review, 116, 105188. DOI https://doi.org/10.1016/j.childyouth.2020.105188
Gotch, K., & Hanson, R. K. (2016). Risk assessment for males who have engaged in harmful or illegal sexual behavior. Beaverton, OR, USA: Association for the Treatment of Sexual Abusers. static1.squarespace.com https://static1.squarespace.com/static/5cfac957e859ec000154b8a7/t/5d0a807297cc0500018d2837/1560969332831/ATSA_Risk_Assessment_for_Males_(2016)+(1).pdf
Greater Manchester Safeguarding. (2022). Harmful sexual behaviours presented by children and young people. In Greater Manchester Safeguarding Children Procedures Manual. Lancashire, UK: Greater Manchester Safeguarding. greatermanchesterscp.trixonline.co.uk https://greatermanchesterscp.trixonline.co.uk/chapter/harmful-sexual-behaviours-presented-by-children-and-young-people
Hackett, S. (2014). Children and young people with harmful sexual behaviours: Research review. London, UK: Research in Practice. tce.researchinpractice.org.uk https://tce.researchinpractice.org.uk/wp-content/uploads/2020/05/children_and_young_people_with_harmful_sexual_behaviours_research_review_2014.pdf
Hackett, S., Branigan, P., & Holmes, D. (2019). Harmful sexual behaviour framework: An evidence-informed operational framework for children and young people displaying harmful sexual behaviours. London, UK: NSPCC. learning.nspcc.org.uk https://learning.nspcc.org.uk/media/1657/harmful-sexual-behaviour-framework.pdf
Hackett, S., Phillips, J., Masson, H., & Balfe, M. (2013). Individual, family and abuse characteristics of 700 British child and adolescent sexual abusers. Child Abuse Review, 22(4), 232–245. DOI https://doi.org/10.1002/car.2246
Hart, S. D., & Boer, D. P. (2021). Structured professional judgement guidelines for sexual violence risk assessment. In K. S. Douglas & R. K. Otto (Eds). Handbook of violence risk assessment. 2nd edn. (pp. 322–358). New York, USA: Routledge. DOI https://doi.org/10.4324/9781315518374-18
Jensen, M., Askeland, I. R., & Bjorknes, R. (2022). Interrater reliability and experiences of assessment, intervention, and moving-on 3 assessment model in a multidisciplinary Norwegian sample. Frontiers in Psychology, 13, 1019739. DOI https://doi.org/10.3389/fpsyg.2022.1019739 PMid:36544449
Jung, S., & Thomas, M. L. (2022). A compendium of risk and needs tools for assessing male youths at-risk to and/or who have engaged in sexually abusive behaviors. Sexual Offending: Theory, Research, and Prevention, 17, e8085. DOI https://doi.org/10.5964/sotrap.8085
Kang, T., Beltrani, A., Manheim, M., Spriggs, S., Nishimura, B., Sinclair, S., Stachniuk, M., Pate, E., Righthand, S., Worling, J. R., & Prentky, R. A. (2019). Development of a risk/treatment needs and progress protocol for juveniles with sex offenses. Translational Issues in Psychological Science, 5(2), 154–169. DOI https://doi.org/10.1037/tps0000191
Langton, C. M., Awrey, M. J., & Worling, J. R. (2023). Protective factors in the prediction of criminal outcomes for youth with sexual offenses using tools developed for adults and adolescents: Tests of direct effects and moderation of risk. Psychological Assessment, 35(6), 497–509. DOI https://doi.org/10.1037/pas0001227 PMid:36862457
Liddle, C., Gray, P., Burton, J., Kumar, R., Tunny, T., Prideaux, C., Armstrong, E., McCracken, A., French, B., Attenborough, I., Wolfe, H., Harris, L., Lally, D., Corrales, T., Krakouer, J., Beaufils, J., & Behrendt, L. (2022). The family matters report 2022. Yálla-birr-ang/Collingwood: SNAICC. apo.org.au https://apo.org.au/node/320961
Mathews, B., Finkelhor, D., Pacella, R., Scott, J. G., Higgins, D. J., Meinck, F., Erskine, H. E., Thomas, H. J., Lawrence, D., Malacova, E., Haslam, D. M., & Collin-Vézina, D. (2024). Child sexual abuse by different classes and types of perpetrator: Prevalence and trends from an Australian national survey. Child Abuse & Neglect, 147, 106562. DOI https://doi.org/10.1016/j.chiabu.2023.106562 PMid:38061281
McKibbin, G., Humphreys, C., Tyler, M., & Spiteri-Staines, A. (2022). Clusters of risk associated with harmful sexual behaviour onset for children and young people: Opportunities for early intervention. Journal of Sexual Aggression, 30(2), 185–196. DOI https://doi.org/10.1080/13552600.2022.2117429
McKillop, N. (2018). Bravehearts Turning Corners Program: A short-term outcome evaluation. Gold Coast: Bravehearts.
Miccio-Fonseca, L. C. (2018). Family lovemap and erotically related protective factors. Journal of Child Sexual Abuse, 27(8), 901–917. DOI https://doi.org/10.1080/10538712.2018.1494655 PMid:30064305
Miccio-Fonseca, L. C. (2023). Setting the record straight regarding tools that assess risk for youth with sexually abusive behavior. Journal of Child Sexual Abuse, 33(1), 102–125. DOI https://doi.org/10.1080/10538712.2023.2280027 PMid:37994404
Miccio-Fonseca, L. C., & Rasmussen, L. A. (2015). MEGA♪ – Empirical support for nomenclature on the anomalies: Sexually violent and predatory youth. International Journal of Offender Therapy and Comparative Criminology, 59(11), 1222–1238. DOI https://doi.org/10.1177/0306624X14533265
Miccio-Fonseca, L. C., & Rasmussen, L. A. L. (2018). Scientific evolution of clinical and risk assessment of sexually abusive youth: A comprehensive review of empirical tools. Journal of Child Sexual Abuse, 27(8), 871–900. DOI https://doi.org/10.1080/10538712.2018.1537337 PMid:38061281
Miccio-Fonseca, L. C., & Rasmussen, L. A. L. (2020). Sexually abusive youth with low intellectual functioning: contemporary risk assessment findings from MEGA♪ studies. Journal of Aggression, Maltreatment & Trauma, 29(8), 1000–1019. DOI https://doi.org/10.1080/10926771.2019.1660444
Molnar, T., Allard, T., McKillop, N., & Rynne, J. (2022). Reliability and predictive validity of the Juvenile Sex Offender Assessment Protocol-II in an Australian context. International Journal of Offender Therapy and Comparative Criminology, 66(10–11), 1051–1070. DOI https://doi.org/10.1177/0306624X19900978 PMid:31957511
Myers, S. (2007). (De)constructing the risk categories in the AIM assessment model for children with sexually harmful behaviour. Children & Society, 21(5), 365–377. DOI https://doi.org/10.1111/j.1099-0860.2006.00053.x
National Society for the Prevention of Cruelty to Children. (2021). Statistics briefing: Harmful sexual behaviour. London, UK: NSPCC. learning.nspcc.org.uk https://learning.nspcc.org.uk/media/1661/statistics-briefing-harmful-sexual-behaviour.pdf
Navarro, J. L., & Tudge, J. R. H. (2022). Technologizing Bronfenbrenner: neo-ecological theory. Current Psychology, 42, 19338–19354. DOI https://doi.org/10.1007/s12144-022-02738-3 PMid:35095241
Nolan, M. (2017). Emerging perceptions of effective risk assessment and interventions from expert practitioners working with young people (YP) displaying harmful sexual behaviour (HSB). MSc Thesis. Manchester, UK: Manchester Metropolitan University. DOI https://doi.org/10.13140/RG.2.2.14427.16164
O'Brien, W. (2010). Australia's response to sexualised or sexually abusive behaviours in children and young people. Canberra: Australian Crime Commission. apo.org.au https://apo.org.au/node/22180
Paton, A., Bromfield, L., Moore, T., Ey, L.-A., Burgess, S., Cox, S., Herbert, J. & Department of Communities. (2022). Framework for understanding and guiding responses to harmful sexual behaviours in children and young people. Perth: Australian Centre for Child Protection, Western Australia. wa.gov.au https://www.wa.gov.au/system/files/2022-07/Framework-Understanding-Guiding-Harmful-Sexual-Behaviours.pdf
Powers-Sawyer, A. B., & Miner, M. H. (2009). Actuarial prediction of juvenile recidivism: The static variables of the Juvenile Sex Offender Assessment Protocol-II (J-SOAP-II). Sexual Offender Treatment, 4(2). researchgate.net https://www.researchgate.net/publication/41392393_Actuarial_Prediction_of_Juvenile_Recidivism_The_Static_Variables_of_the_Juvenile_Sex_Offender_Assessment_Protocol-II_J-SOAP-II
Prentky, R. A., & Righthand, S. (2003). Juvenile Sex Offender Assessment Protocol-II (J-SOAP-II) manual. US Department of Justice. proceduresonline.com https://www.proceduresonline.com/bromley/yot/user_controlled_lcms_area/uploaded_files/Sex_Offenders_assessment_J-SOAP_II.pdf
Productivity Commission. (2023). Closing the Gap annual data compilation report July 2023. Canberra: Australian Government. pc.gov.au https://www.pc.gov.au/closing-the-gap-data/annual-data-report/2023/report
Righthand, S., Worling, J. R., Prentky, R. A., & Kang, T. (2020). Youth Needs and Progress Scale & user guide. US Department of Justice. drjamesworling.com https://www.drjamesworling.com/uploads/8/7/7/6/8776493/youth_needs_and_progress_scale_2020.pdf
Rojas, E. Y. (2013). Violence risk assessment with youth who have sexually offended: a psychomatric examination of the Violence Risk Scale: Youth Sexual Offender Version (VRS:YSO). PhD Thesis. Saskatoon, Canada: University of Saskatchewan. core.ac.uk https://core.ac.uk/download/pdf/226154485.pdf
Rojas, E. Y., & Olver, M. E. (2020). Validity and reliability of the Violence Risk Scale-Youth Sexual Offense Version. Sexual Abuse, 32(7), 826–849. DOI https://doi.org/10.1177/1079063219858064 PMid:31248327
Royal Commission into Institutional Responses to Child Sexual Abuse. (2017). Final report: Children with harmful sexual behaviours. Canberra: Australian Government. childabuseroyalcommission.gov.au https://www.childabuseroyalcommission.gov.au/sites/default/files/final_report_-_volume_10_children_with_harmful_sexual_behaviours.pdf
Seto, M. C., & Lalumiere, M. L. (2010). What is so special about male adolescent sexual offending? A review and test of explanations through meta-analysis. Psychological Bulletin, 136(4), 526–575. DOI https://doi.org/10.1037/a0019700 PMid:20565168
Shaw, J. A., Lewis, J. E., Loeb, A., Rosado, J., & Rodriguez, R. A. (2000). Child on child sexual abuse: Psychological perspectives. Child Abuse & Neglect, 24(12), 1591–1600. DOI https://doi.org/10.1016/S0145-2134(00)00212-X PMid:11197037
Taber, K. S. (2017). The use of Cronbach's Alpha when developing and reporting research instruments in science education. Research in Science Education, 48, 1273–1296. DOI https://doi.org/10.1007/s11165-016-9602-2
Tavakol, M., & Dennick, R. (2011). Making sense of Cronbach's alpha. International Journal of Medical Education, 27(2), 53–55. DOI https://doi.org/10.5116/ijme.4dfb.8dfd PMid:28029643
Van Der Put, C. E., Deković, M., Stams, G. J. J. M., Van Der Laan, P. H., Hoeve, M., & Van Amelsfort, L. (2011). Changes in risk factors during adolescence. Criminal Justice and Behavior, 38(3), 248–262. DOI https://doi.org/10.1177/0093854810391757
Vitacco, M. J., Caldwell, M., Ryba, N. L., Malesky, A., & Kurus, S. J. (2009). Assessing risk in adolescent sexual offenders: Recommendations for clinical practice. Behavioral Sciences & the Law, 27(6), 929–940. DOI https://doi.org/10.1002/bsl.909 PMid:19937921
Westerman, T. (2010). Engaging Australian Aboriginal youth in mental health services. Australian Psychologist, 45(3), 212–222. DOI https://doi.org/10.1080/00050060903451790
Worling, J. R. (2017). History & rationale. In PROFESOR: Protective + Risk Observations For Eliminating Sexual Offence Recidivism. profesor.ca https://www.profesor.ca/history--rationale.html
Worling, J. R. (2020). PROFESOR: Protective + Risk Observations For Eliminating Sexual Offence Recidivism user's guide 1.0. profesor.ca https://www.profesor.ca/uploads/8/7/7/6/8776493/profesor_user_guide_1.0_2020.pdf
Worling, J. R., & Langton, C. M. (2012). Assessment and treatment of adolescents who sexually offend: Clinical issues and implications for secure settings. Criminal Justice and Behavior, 39(6), 814–841. DOI https://doi.org/10.1177/0093854812439378
Appendix I